
A practical, prioritized guide for managed care organizations preparing for Health Outcomes and Community-Focused Care Accreditation.
Effective for NCQA surveys on or after July 1, 2026
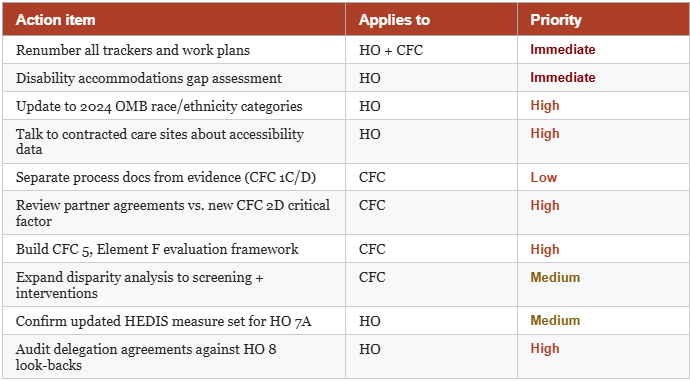
Over the past four blogs, we have walked through every major change in NCQA's 2026 Health Outcomes Accreditation (formerly Health Equity) and Community-Focused Care Accreditation (formerly Health Equity Plus). In this final post, we pull the most important actions into a single prioritized checklist — the ten things your organization should do right now, regardless of where you are in the accreditation cycle.
Some of these items apply to organizations pursuing Health Outcomes Accreditation only. Some are specific to Community-Focused Care. Most apply to both. We have noted which is which.
The organizations that succeed in 2026 NCQA surveys will be the ones that started preparing in 2025. The new requirements — especially disability accommodations and social needs effectiveness evaluation — cannot be assembled at the last minute.
1. Renumber Everything
Applies to: Both HO and CFC
The renaming and renumbering of standards and elements is extensive in both programs. Every internal work plan, gap assessment, scoring tracker, policy reference, and documentation checklist that uses Health Equity or Health Equity Plus numbering (HE 1 through HE 7, HE Plus 1 through HE Plus 5) needs to be updated to the new numbering before your team does anything else.
Working from stale numbering is the most common source of survey preparation errors. A gap that appears closed may actually be open under the new framework. An element your team believes is handled may have split into two. Do the renaming work first, so every subsequent action is oriented to the correct target.
2. Launch a Disability Accommodations Gap Assessment Immediately
Applies to: Health Outcomes Accreditation
HO 4 is an entirely new standard with four elements and no prior equivalent in the Health Equity program. HO 2, Elements D and E require new data collection on disability status and disability-related accommodations. HO 5, Elements D and E require information on accessible equipment and care site accessibility. This is the largest net-new work in the 2026 Health Outcomes standards, and it spans five elements across three standards.
A disability accommodations gap assessment should map your current state in each of these areas: what data you collect, what accommodation processes exist, what your contracted care sites can report, and what your digital content accessibility looks like. Most organizations will find significant gaps. The sooner you know the scope, the more time you have to close it.
3. Update Your Race/Ethnicity Data Collection for 2024 OMB Categories
Applies to: Health Outcomes Accreditation
HO 2, Element A now requires alignment with the 2024 OMB race and ethnicity categories, which reorganized how racial and ethnic groups are categorized and collected. Organizations that built their data collection framework around the pre-2024 OMB standards will need to update their collection tools, scripts, enrollment forms, and any third-party data feeds.
This is not a small administrative update. It may require changes to your electronic data systems (which are separately assessed under HO 2, Element H), your data collection documentation, and your reporting logic. Start by confirming exactly which categories your current system uses and mapping the delta to the 2024 OMB framework.
4. Talk to Your Contracted Care Sites About Accessibility Data
Applies to: Health Outcomes Accreditation
NCQA has confirmed in policy clarification guidance that health plans are responsible for HO 5, Elements A and B, factors 3–4 even if they do not own or operate clinical facilities. If your members receive face-to-face care through your contracted network — and they do — these factors apply to your organization.
This means you need to collect information about accessible equipment and disability accommodations at contracted care sites. Begin provider outreach now to understand what information your network partners can supply, what gaps exist, and how you will document and track this data. The sooner this conversation begins, the better positioned you will be when survey time arrives.
NCQA CONFIRMED
There is no exception from HO 5, Elements A and B, factor 4 for organizations that are not care delivery organizations. NCQA acknowledged the explanation in the standards may be confusing and will issue clarifying language in a future publication — but the requirement stands.
5. Separate Your Social Needs Process Documentation From Your Evidence
Applies to: Community-Focused Care Accreditation
Former HE Plus 1, Element C has been split into two separately scored elements: CFC 1, Element C (Process for Collecting Social Needs Data) and CFC 1, Element D (Evidence of Collecting Social Needs Data). NCQA now evaluates your documented process and your actual evidence of collection as distinct activities with separate scores. This is not a difficult process and is the easiest in this listing.
6. Review Partner Agreements Against the New CFC 2, Element D — Especially the Critical Factor
Applies to: Community-Focused Care Accreditation
CFC 2, Element D (Agreements With Partners to Deliver Resources/Interventions) has been substantially revised. Factor 1 is newly designated as a critical factor — meaning a failure on factor 1 caps your element score at ZERO regardless of how well you perform on all other factors. New factors 2 and 3 have been added. Factor 4 language is revised. Scoring has changed.
Pull every active partner agreement and review it line by line against the updated element requirements. Identify which agreements meet the new factor 1 requirements and which need to be renegotiated or amended. This is the highest-priority compliance gap for any CFC organization with active community-based partnerships.
7. Build Your CFC 5, Element F Evaluation Framework
Applies to: Community-Focused Care Accreditation
CFC 5, Element F — Evaluating Effectiveness of Social Needs Referrals and Interventions — is brand new and requires a programmatic response, not just documentation. Your organization must demonstrate that it evaluates whether social needs referrals and interventions are producing results for members.
Start by defining what effectiveness means for each active social needs program. Identify what data you currently collect on referral completion and intervention outcomes. Map the gaps. Then design evaluation processes — even simple ones — that capture the data you need to answer the question: is this helping? This element requires lead time. Build the framework before the survey window opens, not during it.
8. Expand Your Disparity Analysis to Cover Screening and Interventions
Applies to: Community-Focused Care Accreditation
CFC 5, Element D has been expanded from assessing disparities in referral status to assessing disparities in screening, referrals, and interventions. This is a meaningful increase in scope. Your organization must now examine whether social needs screening is reaching all populations equitably, whether referral rates differ across demographic groups, and whether interventions are delivered and accessed equitably.
Review your current disparity analysis methodology and data infrastructure. Determine whether you have the data to stratify screening and intervention outcomes — not just referral counts — by race, ethnicity, language, and other demographic dimensions. Identify gaps and prioritize closing them before your next survey.
9. Confirm Your HEDIS Stratified Measure Set for HO 7
Applies to: Health Outcomes Accreditation
HO 7, Element A replaces the former five-measure stratified reporting set (COL, CBP, HBD, PPC, WCV) with a new four-measure set. The updated measure specifications are in the 2026 standards. Confirm which measures now constitute the required set, verify your HEDIS reporting capabilities cover those measures, and update any internal reporting schedules or vendor contracts accordingly.
Do not assume continuity with the former five-measure set. At least one measure from the old set has been removed, and the scoring thresholds and exceptions have been revised. Verify the current specifications directly with NCQA HEDIS Tech Specs or through the updated standards.
10. Audit Delegation Agreements Against Updated HO 8 Requirements
Applies to: Health Outcomes Accreditation
All four delegation elements in HO 8 (formerly HE 7) carry revisions to look-back periods and/or scoring. Organizations that delegate health equity or health outcomes program activities should review their current delegation agreements and oversight records to confirm they satisfy the updated requirements.
Pay particular attention to look-back period changes — a delegation agreement or oversight review that satisfied the former HE 7 requirements may fall outside the revised look-back window under HO 8. Do not assume your existing delegation infrastructure is compliant without verification.
A note on CFC delegation: the 2026 standards clarify explicitly in Appendix 2 that Community-Focused Care Accreditation activities may not be delegated. If any CFC activities were previously handled through delegation arrangements, those arrangements must be restructured.
The 2026 Health Outcomes and Community-Focused Care standards represent a meaningful evolution in what NCQA expects from managed care organizations. The organizations that will navigate the transition most successfully are not the ones with the most resources — they are the ones that start early, plan deliberately, and build the new requirements into their quality programs rather than treating them as survey preparation tasks.
We have covered the full landscape across this five-part series. If you have questions about any specific standard, need help prioritizing your gap assessment, or want a readiness review ahead of your next survey, our team is ready to help.
Ready to get started?
Have you benefitted from our five blogs on HO/CFC?
Just think what consulting and training we could do for you! Our consultants specialize in NCQA Health Outcomes and Community-Focused Care Accreditation readiness. Whether you are preparing for your first survey or your renewal, we can help you build a clear, prioritized path to success under the 2026 standards. We’ve met the Health Equity standards for many organizations through three cycles and are now assisting them with movement to HO/CFC.
Explore Tools & Training:
Health Outcomes and Community-Focused Care Training: https://www.managedhealthcareresources.com/health-equity-accreditation-training
Health Outcomes Tools & Templates: https://www.managedhealthcareresources.com/health-equity-templates-tools
Delegation Tools & Templates: https://www.managedhealthcareresources.com/delegation-tools-templates
Gap Assessment Tools:
https://www.managedhealthcareresources.com/tools/gap_assessments
Want to explore your readiness options for NCQA or URAC accreditation? Contact us.
Copyright © 2026 Managed Healthcare Resources, Inc. All Rights Reserved.


